The consistent and accurate record-keeping is paramount in effective counseling. A well-structured counseling progress note provides a detailed account of a client’s sessions, facilitating continuity of care, informed decision-making, and effective treatment planning. A robust ‘Counseling Progress Notes Template’ is an essential tool for therapists, counselors, and social workers alike. This article will explore the key components of a comprehensive progress note, offering guidance on formatting, content, and best practices. Counseling Progress Notes Template – understanding its nuances is crucial for delivering optimal client care. This guide will cover everything from basic structure to advanced considerations, ensuring you create notes that are both informative and professional.
Understanding the Purpose of Counseling Progress Notes
The primary purpose of a counseling progress note is to document the client’s progress during a session. It’s more than just a log; it’s a snapshot of the interaction, highlighting key observations, interventions, and the client’s expressed feelings and goals. It serves as a valuable resource for the therapist, allowing them to assess the effectiveness of treatment, identify areas for adjustment, and communicate with other team members. Without a clear and detailed record, it’s difficult to track client progress and ensure that treatment is aligned with their needs. Furthermore, it’s often required for insurance claims and legal documentation. A thoughtfully crafted progress note demonstrates a commitment to client-centered care and facilitates accountability.
Core Components of a Counseling Progress Note
A typical counseling progress note includes several key sections. Each section should be concise and focused on providing relevant information. Here’s a breakdown of the essential elements:
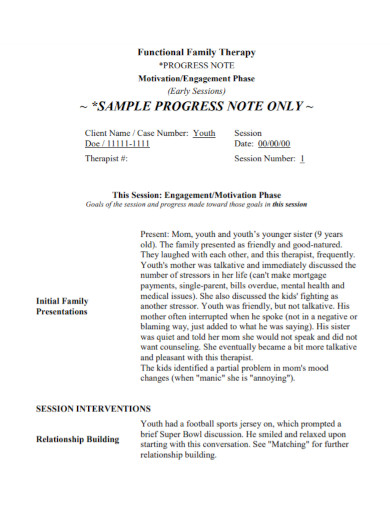
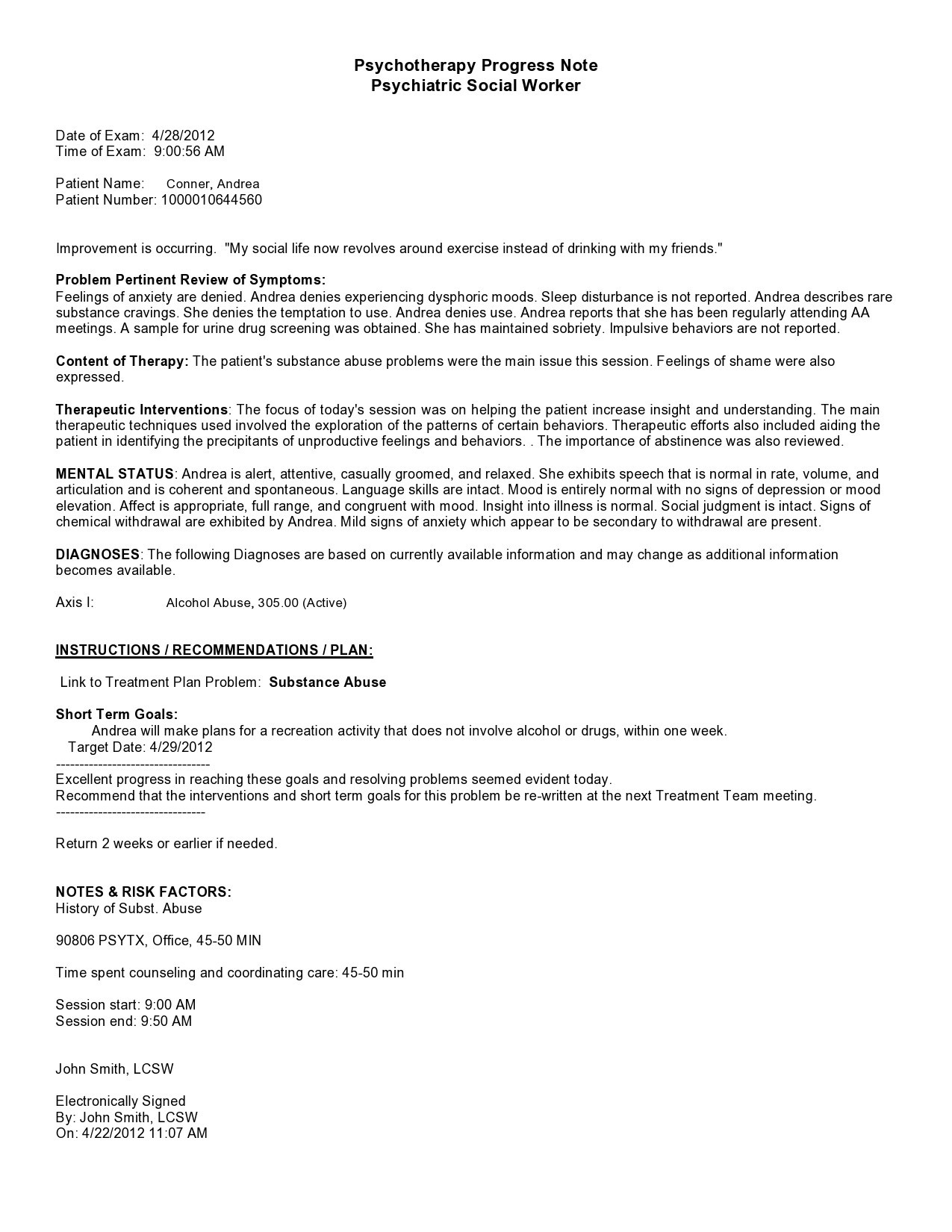
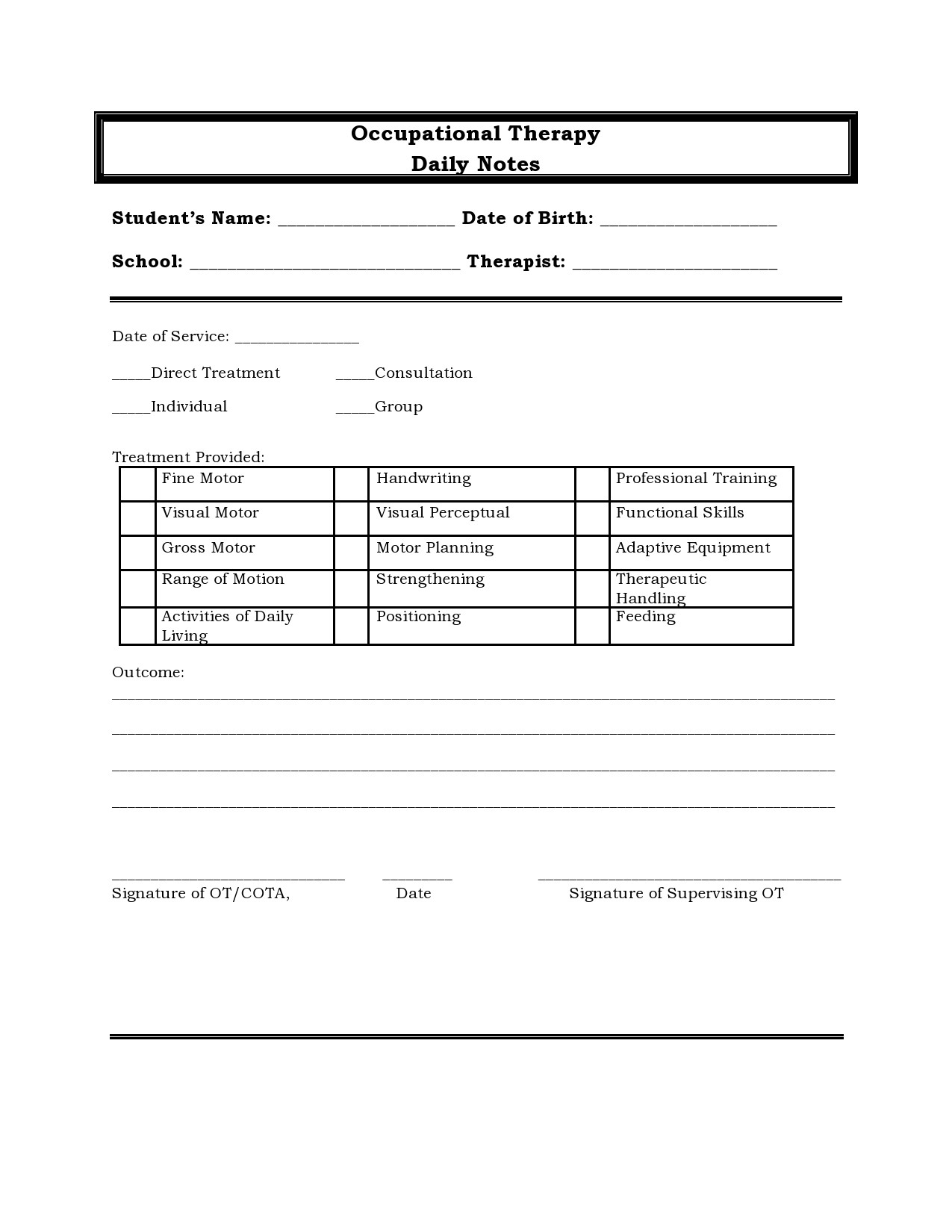
- Client Information: Record the client’s full name, date of birth, and contact information. This ensures easy identification and facilitates communication.
- Session Date and Time: Clearly state the date and time of the session.
- Presenting Problem/Issue: Briefly describe the client’s primary concern or issue that brought them to therapy. This provides context for the session.
- Session Summary: A concise overview of what transpired during the session. This should include key topics discussed, interventions used, and the client’s reactions.
- Interventions: Detail the specific techniques or strategies employed during the session. For example, “Client reported feeling anxious about upcoming job interview” or “Client utilized relaxation techniques to manage distress.”
- Client’s Response/Affect: Document the client’s emotional state and how they responded to the interventions. This is crucial for understanding the therapeutic process. Examples include “Client expressed gratitude for the support” or “Client demonstrated increased self-awareness.”
- Goals: Review the client’s stated goals for therapy. Note any progress made towards achieving those goals.
- Plan for Next Session: Outline the anticipated topics and interventions for the next session. This demonstrates proactive planning and sets the stage for continued progress.
- Therapist’s Comments/Observations: This is where the therapist’s subjective assessment of the session is recorded. This section allows for a more detailed and nuanced account of the interaction.
Structuring Your Counseling Progress Note: A Detailed Guide
A well-organized progress note is easier to read and understand, both for the therapist and the client. Here’s a suggested structure:

1. Initial Section (Top of the Page):
- Client Information: (As mentioned above)
- Session Date & Time: (Clearly displayed)
- Presenting Problem/Issue: (Briefly stated)
2. Session Summary (2-3 Paragraphs):
- Key Events: A bulleted list of the most important events of the session.
- Interventions Used: Briefly describe the interventions employed.
- Client’s Reactions: Summarize the client’s emotional responses.
3. Detailed Section – Interventions & Client Response (Most Important Section):
- Detailed Description: Provide a thorough explanation of the interventions used. Be specific about how the therapist implemented the intervention.
- Client’s Response: Document the client’s reaction to each intervention. Use descriptive language to illustrate the client’s experience. For example, “Client demonstrated increased engagement with the discussion about their childhood trauma.”
- Impact of Intervention: Assess the impact of the intervention on the client’s emotional state and behavior.
4. Goals & Progress (1-2 Paragraphs):
- Review of Goals: Restate the client’s stated goals.
- Progress Towards Goals: Describe any progress made towards achieving those goals. Be specific and quantifiable if possible. For example, “Client reported feeling more confident in their ability to manage stress” or “Client successfully identified three potential coping mechanisms.”
5. Plan for Next Session (1-2 Paragraphs):
- Topics to Discuss: List the topics to be addressed in the next session.
- Interventions: Outline the anticipated interventions.
- Client’s Concerns/Questions: Note any concerns or questions the client may have.
6. Therapist’s Comments/Observations (2-3 Paragraphs):
- Overall Impression: Provide a brief summary of the session’s overall effectiveness.
- Strengths: Highlight any strengths of the client’s presentation or the therapeutic process.
- Areas for Consideration: Note any areas where the client’s presentation or the therapeutic approach could be improved.
Advanced Considerations and Best Practices
- Objectivity: Maintain a professional and objective tone. Avoid expressing personal opinions or judgments. Focus on factual observations.
- Specificity: Use concrete language and avoid vague descriptions. Instead of saying “Client seemed upset,” write “Client exhibited signs of distress, including fidgeting and a downturned expression.”
- Documentation: Maintain a detailed and accurate record of all sessions.
- Legal Considerations: Be mindful of privacy regulations and confidentiality requirements. Only record information that is relevant to the client’s treatment.
- Electronic Progress Notes: Many therapists now utilize electronic progress note systems. Ensure your system is properly formatted and compliant with HIPAA regulations.
- Client Input: Encourage clients to provide feedback on the progress note. This can help ensure that the notes are accurate and helpful.
Conclusion
The counseling progress note is a vital component of effective therapy. By following a structured approach and paying attention to detail, therapists can create notes that provide a comprehensive and informative record of the client’s progress. A well-crafted progress note facilitates continuity of care, informs treatment planning, and ultimately contributes to improved client outcomes. Remember that the goal is to accurately and objectively document the client’s experience, supporting informed decision-making and promoting positive change. Counseling Progress Notes Template – consistently utilizing this template will significantly enhance your therapeutic practice.